

TONGUE TIE
Tongue tie (also known as ankyloglossia, tight lingual frenum/frenulum, or tethered oral tissue/TOTS) is when the tissue that connects the underside of the tongue to the floor of the mouth is restricted, causing limitations to the function of the tongue. It is important to understand that tongue ties can range from mild to severe and present differently in every person.
A thorough assessment is necessary (its not as simple as poking your tongue out) to determine whether there are functional issues, as not all tongue ties require a tongue tie release (surgery).
Signs and symptoms that you or your child may have a tongue tie?
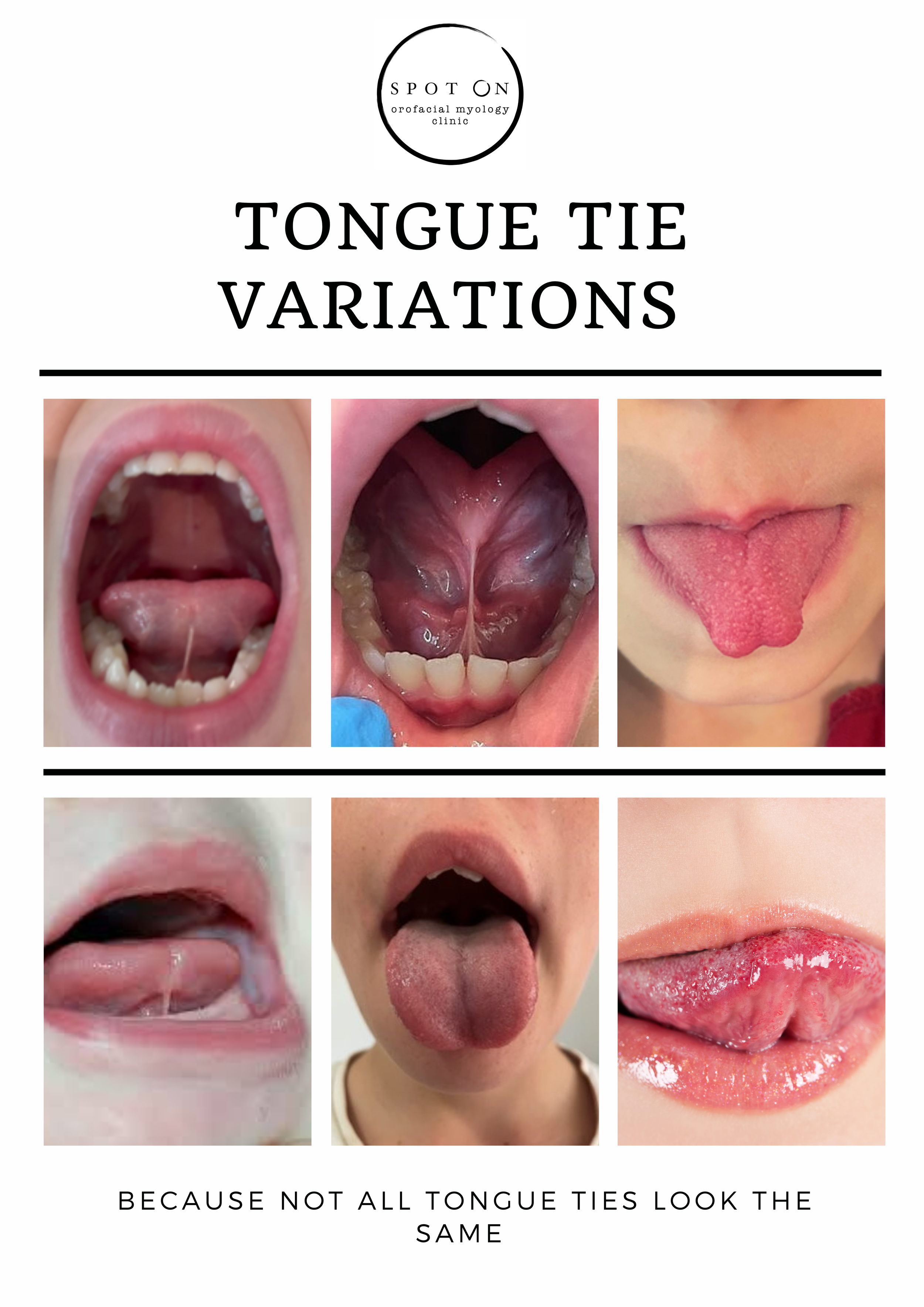
A heart shaped tip when sticking the tongue out
A block shaped tongue when sticking the tongue out
Inability to lick an ice cream
Impaired speech (articulation)
Slow eater
Selective eating (avoiding foods that are difficult to chew, like meat)
Sleep Disordered Breathing
Headaches
Jaw pain
Tongue chewing
Breastfeeding issues as an infant, including difficulty with latch/low supply/falling asleep on the breast/mastitis
High incidence of dental decay and gum disease (even with good oral hygiene practices and good diet)
Digestive issues- the tongue needs to be fully functioning to allow for optimal chewing, and for salivary enzymes to enter the food as the first phase of digestion. Consitpation, bloating and passing of gas can be caused by suboptimal chewing
REMEMBER!
The position of the tongue is important for jaw and facial growth in children.
If the tongue is significantly restricted in its movement and is unable to seal in the palate at rest because it is tied to the floor of the mouth, the jaws are more likely to be narrower, and teeth more crowded.

how is a tongue tie released?
Laser surgery is the preferred way to treat tongue and lip ties, vaporising the frenum layer by layer until it is released. This method is preferred over cutting the frenum with scissors/scalpel as the laser causes ablation (‘taking away’ of tissue) to occur which means there is little to no bleeding, and it reduces the risk of infection. It is a relatively quick and straightforward process performed in the dental chair, with no stitches required. It can be done with local or topical anaesthetic, and in most cases a general anaesthetic is not necessary.
Your tongue/lip tie release provider will provide you with further information regarding this.
How this relates to orofacial myology…
The whole point of having tongue tie release surgery (frenectomy/frenuloplasty) is to improve the function of the tongue and other orofacial muscles. For this to occur, orofacial myofunctional therapy is required to get the BEST OUTCOME from a tongue tie release, because its not a cosmetic procedure- its all about FUNCTION!
The goal of orofacial myofunctional therapy in relation to tongue tie release:
Improve the strength and tone of the tongue
Improve the range of motion of the tongue
Correct oral resting posture, so that the tongue is suctioned to the palate at rest
Eliminate compensatory patterns
Stabilise the jaw (when the tongue is tied, the jaw does a lot of the moving as the tongue is unable to dissociate from the jaw easily)
Establish nasal breathing with lip seal
Establish bilateral chewing with lip seal (when the tongue is tied it can be difficult to move food around the mouth and chewing can be tiring)


The importance of tongue tie release in conjunction with orofacial myofunctional therapy
A large 2019 study of 348 patients who had tongue tie release surgery AND orofacial myofunctional therapy showed:
Satisfaction rate of 91%
Improvements in mouth breathing (78.4%)
Snoring (72.9%)
Clenching (91%)
Myofascial tension (77.5%)
“Lingual frenuloplasty WITH myofunctional therapy is safe and potentially effective for the treatment of mouth breathing, snoring, clenching, and myofascial tension in appropriately selected patient candidates.”
the research…
Lingual Frenuloplasty with Myofunctional Therapy: Exploring safety and efficacy in 348 cases
A frequent phenotype for paediatric sleep apnoea: short lingual frenulum
Short lingual frenulum and head-forward posture in children with the risk of obstructive sleep apnea
Short lingual frenulum as a risk factor for sleep-disordered breathing in school-age children
Speech and Feeding Improvements in Children After Posterior Tongue-Tie Release: A Case Series