

Dental and orthodontic concerns
Malocclusion
A malocclusion is when your teeth do not meet correctly when you bite together.
Malocclusions do not just affect the way you look when you smile, they can also cause:
Excessive tooth wear
Pain in your jaw joints and facial muscles
Difficulty with eating and speaking
An increased risk of dental trauma
An increased risk of dental decay and periodontal disease


early intervention ORTHODONTICS
versus
Traditional orthodontics
Early intervention orthodontics
Early intervention orthodontics, also known as functional or early interceptive orthodontics takes advantage of a child’s active growth phase to re-establish normal facial growth. This is undertaken to reduce the need for the extraction of permanent teeth whilst creating a good looking facial profile and smile, and a healthy airway.
Children aged between approximately 5-11 years can benefit significantly from this type of treatment as their jaw bones are still soft and easily pliable and there is a window of growth to utilise.
Its important to note that:
→ 60% of a child’s facial development is completed by age 8
→ 90% of a child’s facial development is completed by age 12
Early intervention orthodontics is usually done using an expander (plate). A key is turned every few days (this is dependant on the type of plate, age of child and treatment needs) which opens the expander placing pressure on the bone. The bone then remodels forming a wider jaw. This allows space to accommodate the teeth, and improves the nasal airway. Children aged between approximately 5-11 years can benefit significantly from this type of treatment as their jaw bones are still soft and easily pliable.
→
→
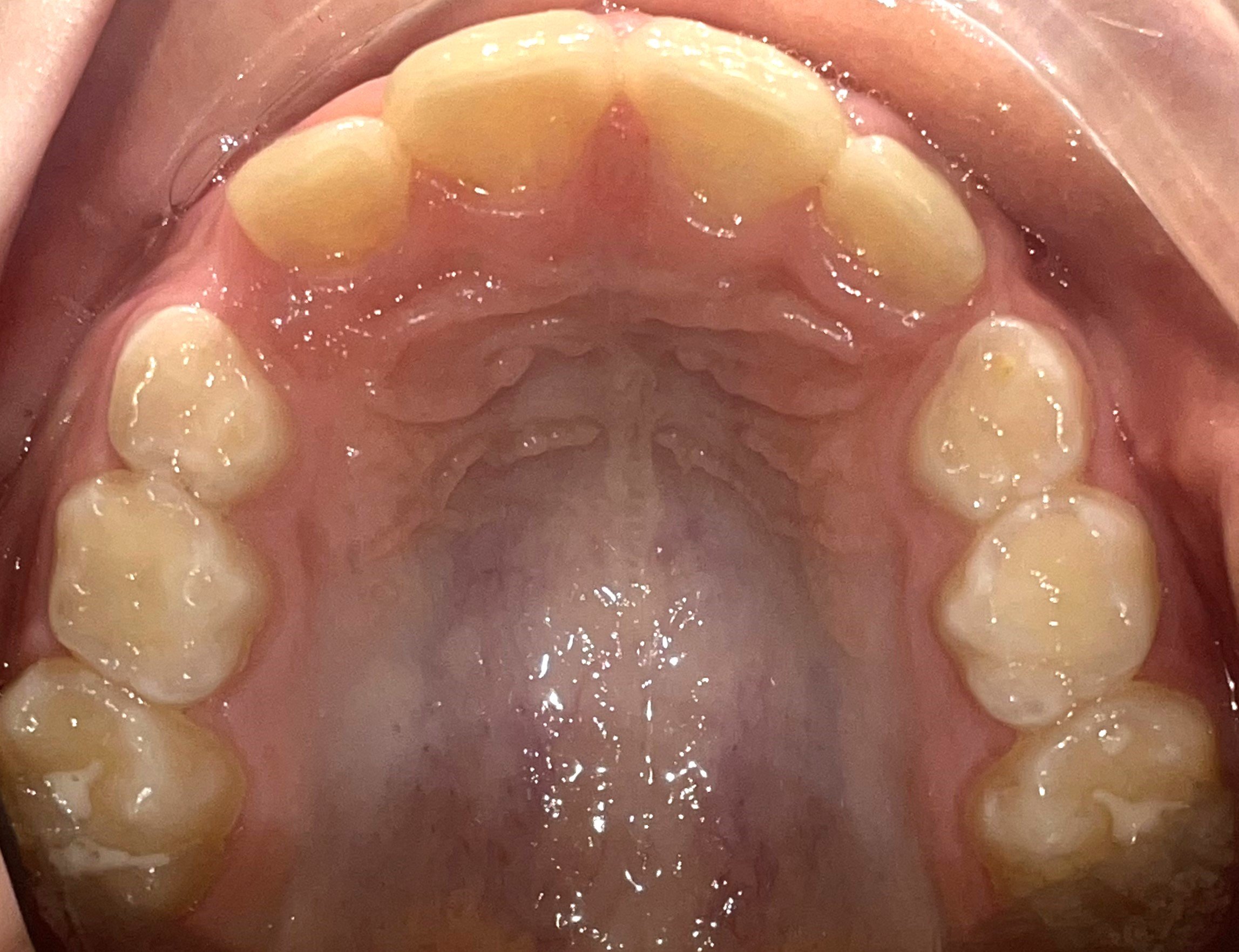
Prior to expansion:
Note the black arrows pointing to the space where the permanent canines (“eye teeth”) need to erupt. Without expansion of the jaw, these teeth would not have the space to erupt. If left, this child would most likely have permanent teeth extracted to make space and then braces to pull the canines down into the position where the teeth were extracted from.

EARLY INTERVENTION Expansion:
The image above shows 7mm of expansion in a 10 year old. creating space for the canine (“eye teeth”). The central mechanism on the plate is turned using a ‘key’ daily over a period of 3-6 months.
Traditional orthodontics
The traditional style of treatment offered by many Specialist Orthodontists for dental crowding is quite different to that of early intervention orthodontics. With traditional orthodontics, treatment doesn’t usually begin until all of the permanent teeth have erupted and the majority of growth is complete. This is usually around twelve years of age. If at this point there is significant dental crowding because the jaws haven’t grown enough to accommodate all of the permanent teeth, the premolars are often extracted to make space for the remaining teeth. Braces (or in some cases Clear Aligners) are then used to align and straighten the teeth.

Why do we prefer Early Intervention Orthodontics?
“Appropriate early treatment is an effective interceptive measure that lays the foundation for a healthy and well-functioning mouth in adulthood.”
The benefits of
early intervention orthodontics:
→ Reduction in dental crowding and space concerns
→ Decreases the likelihood of future extensive orthodontic treatment
→ Decreases the amount of time wearing braces, and in some cases eliminates the need for braces
→ The prevention of impacted teeth and potential damage they may cause to adjacent teeth
→ Reduces the risk of nerve damage to teeth from extensive movement through the bone with braces
→ The elimination of jaw shifts/deviations which may lead to TMJ (jaw joint) issues
→ Works with the child’s natural growth patterns to achieve a well developed cranio-facial base (foundation)
→ Improved breathing patterns and a reduction in sleep disordered breathing/sleep apnoea
The Australian Society of Orthodontists recommends an assessment for early intervention by the age of seven.

The aim of orthodontic treatment should not just be on straightening teeth
It is imperative that we are also developing healthy airways and balanced facial profiles
The Benefits of Orofacial Myofunctional Therapy in conjunction with early interceptive Orthodontic Treatment
Prior to the commencement of any orthodontic treatment, it is imperative that any orofacial myofunctional disorders have been recognised and appropriately treated.
There are two main causes of malocclusions; Genetics, and Orofacial Myofunctional Disorders. Whilst we can’t change our genes, we can address the Orofacial Myofunctional Disorders and the earlier we do this, the better. The goal of orthodontics should not just be to create straight teeth, but also to create a healthy airway & temporomandibular joint, and an attractive facial profile.
We need to start at the start, and where possible CORRECT the CAUSE of the malocclusion early, aiming to create a healthy foundation;
rather than dealing with the result of the problem (the crowded teeth and malocclusion) when the majority of the child’s growth is complete and treatment planning options are limited and often consists of extraction of permanent teeth.
When the muscles of the face and mouth are working optimally, and there is the correct balance of forces from the tongue, lips, cheeks and jaws we have a stable occlusion.
Correct oral resting posture
♦ Lips sealed
♦ The whole tongue suctioned to the palate (roof of the mouth)
♦ Molar teeth slightly apart (not touching)
When the tongue is resting in the floor of the mouth it is no longer balancing out the pressure the cheek muscles are exerting on the sides of the jaws, preventing the natural growth of the jaws. In many cases this causes the development of narrow, under developed and restricted jaws, which leads to crowded teeth.
The tongue must be resting in the roof of the mouth, pushing the palate from the inside out to develop a U-shaped structure that fits all of the teeth. If you mouth breathe, your tongue will naturally rest in the floor of your mouth.


For more information visit The Breathe Institute